- Research
- Open access
- Published:
Retrospective study of congenital airway malformations detected by flexible fiberoptic bronchoscopy in Alexandria University Children’s Hospital
The Egyptian Journal of Bronchology volume 17, Article number: 31 (2023)
Abstract
Background
Congenital airway malformations affect the quality of life and increase the family burden. The care of children who have these lesions requires considerable expenditures of time and other resources within a tertiary care center.
Aim
This work aims to determine the incidence of congenital airway malformations in children with airway-related manifestations detected by flexible fiberoptic bronchoscopy at the bronchoscopy unit of Alexandria University Children Hospital during the period from 1st of January 2019 to 31st of December 2019.
Patients and methods
This retrospective study includes symptomatic children who underwent flexible fiberoptic bronchoscopy from 1st of January 2019 to 31st of December 2019.
Results
The incidence of congenital airway malformations in the studied population was 32%. The mean age of patients at time of diagnosis was 7 months and the most common congenital anomaly was laryngomalacia.
Conclusion
We concluded that congenital airway malformations are not uncommon in newborns and their early detection can be beneficial for optimum management.
Introduction
Congenital airway malformations are heterogeneous congenital respiratory disorders. They have been reported with an incidence of 0.1 to 2% in the population. Inherent to airway anomalies is high morbidity and mortality, the need for specialized chronic care, disproportionate allocation of resources, and a poor quality of life. Intensive care units for neonates and children care for an increasing number of children with these types of airway problems [1, 2]. Diagnostic evaluation should include detailed antenatal history, clinical history, and physical examination. Further investigations will be needed if the following signs and symptoms are present including; recurrent stridor or wheeze, chronic cough, recurrent cyanotic episodes, life-threatening events, feeding difficulties with failure to thrive, failure of extubation, associated other congenital anomalies, and repeated chest infections [3, 4].
Investigations include plain X-rays, laryngoscopy, bronchoscopy, CT scan, and Magnetic resonance image (MRI). Imaging techniques are extremely helpful both pre and post-endoscopy or when endoscopy is not feasible [3,4,5].
A bronchoscopy is an indispensable tool in the clinical evaluation and management of pediatric airway disease. It is a minimally invasive and superior technique for directly visualizing and evaluating airway anatomy and mucosa compared with chest radiography, high-resolution CT scan, and bronchogram. It allows direct visualization of airways either by rigid bronchoscope (RB) or flexible fiberoptic bronchoscope (FFB). There are no absolute contraindications for bronchoscopy; however, suitable indications, appropriate equipment, and skilled personnel are mandatory to perform a safe procedure [6, 7].
The major advantages of FFB as compared to RB include the smaller external diameter of the new pediatric flexible scopes, the ability to change direction within the airway, fine illumination with fiberoptic technology, and airway dynamics evaluation. Detailed inspection of dynamics is critical in diagnosing certain airway abnormalities. It also allows direct examination of the internal surface of the airways, their diameter, and characteristics of the tracheal and bronchial mucosa, and respiratory tract secretions [7].
Congenital airway malformations affect the quality of life and increase the family burden. The care of children who have these lesions requires considerable expenditures of time and other resources within a tertiary care center [8, 9].
This study aimed to determine the incidence of congenital airway malformations in children with airway-related manifestations with attention to the time of referral of infant, need for hospitalization, associated comorbidities, and outcome. It could help parents and physicians to pay particular attention to this clinical condition and improve health care quality.
Patients and methods
This retrospective study included symptomatic children who underwent flexible fiberoptic bronchoscopy in the bronchoscopy unit of Alexandria University Children’s Hospital from 1st of January 2019 to 31st of December 2019. The initial source for patient identification is a retrospectively kept database (Microsoft Access 2007) of the bronchoscopy unit. Collected data included: Demographic data, antenatal and perinatal history, history of hospitalization and ventilation, source of referral, the onset of manifestations, presenting manifestations, associated co-morbidities, investigations, the technique of bronchoscopy, and anesthesia, bronchoscopic finding, treatment and outcome.
Inclusion criteria
Patients with onset of airway-related symptoms less than 3 months of age.
Exclusion criteria
-
1.
Patients with onset of symptoms beyond the age of three months will be excluded.
-
2.
Patients with incomplete medical records and data will be excluded.
The reference practice for bronchoscopy practice, indications, diagnostic utility, safety, necessary equipment and methodology of this procedure have been described [10].
In the studied cases, bronchoscopy was done through a laryngeal mask, with general anesthesia and spontaneous breathing with pre-medications.
Two types of FFB were used:
-
1.
Olympus video bronchoscope (4.1 and 4.9 mm external diameter).
-
2.
KARL STORZ–ENDOSKOPE (2.8 mm external diameter).
Olympus bronchoscope was used in all patients while STORZ was used in 3 cases due to narrowing of airways.
The following classifications were used in diagnosis of cases:
-
1.
Onley’s classification of Laryngomalacia as shown in Fig. 1 [11]
-
Type I—prolapse of the mucosa overlying the arytenoid cartilages.
-
Type II—short aryepiglottic folds.
-
Type III—posterior displacement of the epiglottis.
Fig. 1 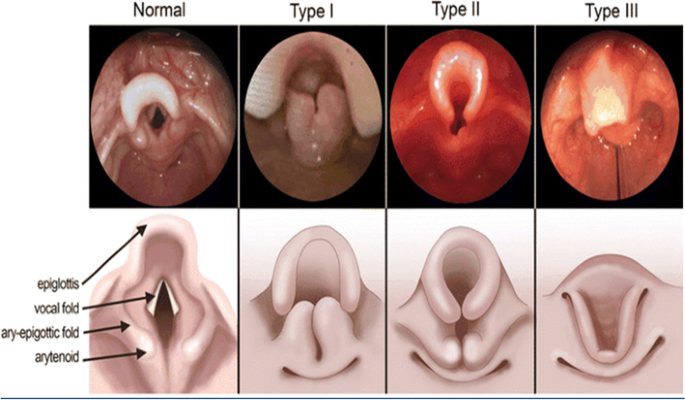
Olney’s classification of laryngomalacia [11]
-

Benjamin and Inglis’s anatomical classification of laryngeal clefts as seen in Fig. 2 [12]:
-
Type I: Supraglottic inter-arytenoid cleft extending to the true vocal folds but not below them.
-
Type II: Partial cricoid cleft that extending to the posterior cricoid cartilage, but not through it.
-
Type III: Total cricoid cleft that may extend to the cervical trachea.
-
Type IV: Cleft extending to the thoracic trachea. Type IV long is a rare variant extending to or beyond the carina.

Benjamin and Inglis classification of laryngotracheal clefts: column A, normal larynx; column B, type I, column C, type II; column D, type III; column E, type IV. The top row is a posterior view, the middle row is a superior view, and the bottom row is an endoscopic intraoperative view [12]
Statistical methodology
Statistical analysis was carried out using IBM SPSS statistics software version 20. (Armonk, NY: IBM Corp.). Qualitative data were expressed by numbers and percentages. The Kolmogrov-Sminrov test was used to verify the normality of distribution. Quantitative data were described using range (minimum and maximum), mean, standard deviation, median, and interquartile range (IQR).
Results
This retrospective study was conducted on symptomatic children who underwent FFB at the bronchoscopy unit of Alexandria University Children’s Hospital. A total of 162 children underwent the FFB procedure during the study period. Congenital airway malformations were detected in 52 patients (incidence 32%). Forty-six cases were included in this study. Six cases were excluded due to incomplete medical records and data.
Table 1 shows that males were more than females. The mean age at the time of diagnosis was 7.59 ± 8.18 months. About the residency, cases from rural were more than urban areas.
Table 2 illustrates that history of intra-cytoplasmic sperm injection was found in one case and, history of maternal illness in 7 cases. Antenatal ultrasound was abnormal in only 5cases. Most cases were born cesarean. Mean gestational age was 38.13 ± 1.57 and mean birth weight was 3.0 ± 0.57.
About resuscitation, routine care in 37% of cases, initial steps in 39%, positive pressure ventilation in 4.34% while endotracheal intubation in 19.6% of cases.
Table 3 shows that manifestations started since birth in the majority of cases (67.4%, no = 31), (15%, no = 7) less than 1 month, and (17.4%, no = 8) from 1 to 3 months of age.
Table 4 illustrates that the most frequent manifestation was stridor. In the majority of cases, multiple manifestations were present while only one manifestation was present in 6 cases; 3 cases presented only with stridor, 2 cases with repeated chest infections, and 1 case with frequent aspirations Figs. 3, 4, 5, 6, 7 and 8.

History of hospitalization. shows that about two-thirds of cases needed hospitalization; 8 cases of them needed more than one hospital admission

History of mechanical ventilation. Illustrates that the majority of cases (59%, no = 27) did not need ventilation while (41.3%, no = 19) needed ventilation

Type III laryngomalacia. Bronchoscopic view of larynx showing collapsing retroflexed epiglottis covering the laryngeal inlet (type III laryngomalacia)

Subglottic stenosis. Bronchoscopic views of subglottic area showing membranous subglottic stenosis causing about 50% narrowing of lumen

Grade III laryngeal cleft. Bronchoscopic view of subglottic area showing grade III laryngeal cleft extending to the lower trachea (black arrow)

Tracheo-esophageal fistula. Bronchoscopic view of trachea showing tracheo-esophageal fistula (arrow) at the level of the carina and at the inlet of the right main bronchus just on the medial aspect of the inlet
Table 5 shows that the most frequent association was cardiac anomalies followed by GERD, hypothyroidism, and cutaneous hemangioma.
Table 6 shows the bronchoscopic findings of the studied cases which were divided into an isolated finding or combined airway malformations. The most frequent anomaly was airway malacia including laryngomalacia and tracheomalacia.
Tables 7 and 8 illustrate the investigations that was done in the studied cases.
Other investigations were done in 27 cases including; plain chest X-ray, high-resolution CT chest with contrast, CT angiography, laryngoscopy, previous bronchoscopy, upper GI endoscopy, and barium study while in 19 cases no further investigations were done.
In 7 cases, bronchoscopic findings were confirmed by radiological investigations.
Table 9 shows that medical treatment was used in about 16 cases and surgical interference was needed in 10 cases, while watchful waiting was enough in 20 cases.
Figure 9 reveals that on follow-up most cases (74%, n = 37) improved while (15%, n = 7) still have manifestations. Mortality occurred in (11%, n = 5) of cases.

Outcome of the studied cases
All cases which did not improve were either planned for surgery or still manifesting after surgery except 2 cases of type III laryngomalacia. Two cases planned for surgery are a case of multiple ring tracheal stenosis and a case of external vascular compression. Three cases seen postoperative were type III laryngomalacia, TEF and grade III laryngeal cleft, and TEF with multiple ring tracheal stenosis.
Cases that died were either preterm with a prolonged hospital stay or cases having associated comorbidities (cardiac anomalies, Down syndrome, and hypothyroidism).
Discussion
Congenital airway malformations include a wide range of anomalies affecting various parts of the airways. They are a major cause of morbidity and mortality that usually manifest and may progress in early life. Due to variable symptoms and clinical course, a high index of clinical suspicion is needed for early diagnosis and management of these lesions [3, 13]. Multiple investigations are now available to identify the diagnosis and quantify the severity of the problem [3, 14]. Bronchoscopy is a minimally invasive and superior technique for direct visualization and evaluation of airway anatomy and mucosa compared with other investigations [7, 15, 16].
Among the studied cases of Bronchoscopy Unit of Alexandria University Children’s Hospital, congenital airway malformations were observed in 35.8% of cases, 46 cases were included in the study.
In this study, the mean age of patients was 7 months and the youngest age was 8 days. Statistical analysis revealed a non-significant difference regarding the sex or residence of the patients.
Hamouda et al. and Sachdev et al. found in their studies that males are more commonly affected than females and the mean age was above 6 months which disagrees with our results [15, 16].
Moslehi et al. found that there is no significant difference regarding the sex of patients in agreement with our findings [17].
The onset of clinical manifestations in about two-thirds of cases started since birth. Multiple manifestations were found in a large percentage of cases but the most common presentation was stridor followed by frequent aspiration and feeding intolerance.
Erdem and his colleagues, (2013) [18], in their study, found that the onset of manifestations in most cases was since birth in agreement with our results. Stridor was present in all of their studied cases followed by wheezes and hoarseness of voice which disagree with our findings.
El Meazawy et al. (2020) [19]. A recent study of central airway collapse in pediatrics in Eygpt found that stridor is a frequent presenting manifestation which agree with the findings of this study.
According to this study results, congenital airway malformations were associated with other co-morbidities in about two-fifth of cases. Congenital heart disease was the most common comorbidity observed in the studied cases.
Inconsistent with this study Lee et al. and scandev et al. found that the most common comorbidity associated with congenital airway anomalies was cardiac anomalies [20, 21].
Bronchoscopic findings revealed that laryngeal anomalies were the most common finding followed by tracheal anomalies. Type III laryngomalacia was the most common laryngeal anomaly followed by laryngeal cleft and subglottic stenosis while the most common tracheal anomaly was tracheomalacia.
Meslehi et al. and Midyat et al. found that malacic disorders were the most common findings which run in line with our results [17, 21].
Guillemaud et al. found that in their studied cases the most frequent bronchoscopic finding were malacic disorders which agree with our results but the most common malacic disorder was tracheomalacia which conflicts with the other study results [22].
The limitations of this work are as follows: first, the retrospective nature of the study resulted in the exclusion of some cases due to missing data. Second, the short duration of the study compared to other studies. Third, our population of children with airway malformations is highly selected and, therefore, is not entirely representative of the general population of children. However, it gives an insight into patients who should probably be referred to pulmonology centers.
Conclusions
From the present study, it can be concluded that congenital airway malformations are not uncommon in newborns and their early detection can be beneficial for optimum management. Airway malformations are a leading cause of morbidity in newborns.FFB can be used as an important diagnostic tool of congenital airway malformations that can guide medical and surgical interventions. Surgical intervention is not the commonly used treatment of congenital airway malformations. Watchful waiting and medical treatment are needed in the majority of cases.
Recommendations
From the present study, we recommend a complete filing system and regular follow-up of such cases will be helpful in further studies. Conducting this study on a larger scale and multicentric basis is needed in the future for further verification of these results. Raising awareness of neonatologists about congenital airway malformations and the importance of FFB is important for early diagnosis and management.
Availability of data and materials
All data generated or analyzed during this study are included in as Supplementary information files.
References
Lee YS, Jeng MJ, Tsao PC, Soong WJ, Chou P (2015) Prognosis and risk factors for congenital airway anomalies in children with congenital heart disease: a nationwide population-based study in Taiwan. PLoS ONE 10(9):e0137437
Azizkhan RG (2020) Congenital airway malformations. Puri P.Pediatric Surgery: General Principles and Newborn Surgery. Springer, Berlin, pp 715–31
Mok Q (2017) Airway problems in neonates—a review of the current investigation and management strategies. Front Pediatr 30(5):60
Vijayasekaran D, Kalpana S, Ramachandran P, et al (2012) Indications and Outcome of Flexible Bronchoscopy in Neonates. Indian J Pediatr 79:1181–1184. https://doi.org/10.1007/s12098-011-0595-6
Tracheobronchial intervention in children (2005) Eur J Radiol 53(1):22–34
Jacobs IN. Bronchoscopy. In: Mattei P. editor. Fundamentals of pediatric surgery. New York: Springer, 2011; 185–94.McLaren CA, Elliott MJ, Roebuck DJ.
Yin Y, Yuan S, Zhong W, Ding Y (2012) Utility of pediatric flexible bronchoscopy in the diagnosis and treatment of congenital airway malformations in children. Global Perspect Bronchoscopy 219:220–240
Lee K-L, Chen T-J, Jeng M-J, Lee Y-S, Tsao P-C, Soong W-J (2016) Laryngotracheobronchial anomalies in infants and the related risk factors of in-hospital mortality. J Chin Med Assoc 79(4):221–227
Masters IB (2009) Congenital airway lesions and lung disease. Pediatr Clin North Am 56(1):227–242
Green CG, Eisenberg J, Leong A, Nathanson I, Schnapf BM, Wood RE (1992) Flexible endoscopy of the pediatric airway. Am Rev Respir Dis 145(1):233–235. https://doi.org/10.1164/ajrccm/145.1.233. (PMID: 1731588)
Reinhard A, Gorostidi F, Leishman C, Monnier P, Sandu K (2017) Laser supraglottoplasty for laryngomalacia; a 14 year experience of a tertiary referral center. Eur Arch Otorhinolaryngol 274(1):367–374
Benjamin B, Inglis A (1989) Minor congenital laryngeal clefts: diagnosis and classification. Ann Otol Rhinol Laryngol 98(6):417–420
Contreras Estay I, Vega-Briceño LE, Sánchez I (2020) Congenital Malformations of the Airway. In: Bertrand P, Sánchez I, editors. Pediatric Respiratory Diseases. Springer, Cham. https://doi.org/10.1007/978-3-030-26961-6_53
Maughan EF, Butler C, Hewitt R, De Coppi P (2021) Pediatric Surgical Diseases of the Larynx, Trachea, and Bronchi. In: Lacher M, St. Peter SD, Zani A, editors. Pearls and Tricks in Pediatric Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-51067-1_12
Sachdev A, Chhawchharia R, Gupta D, Gupta N (2019) Flexible fiberoptic bronchoscopy directed interventions in neonatal intensive care unit. Indian Pediatr 56(7):563–565
Hamouda S, Oueslati A, Belhadj I, Khalsi F, Tinsa F, Boussetta K (2016) Flexible bronchoscopy contribution in the approach of diagnosis and treatment of children’s respiratory diseases: the experience of a unique pediatric unit in Tunisia. Afr Health Sci 16(1):51–60
Moslehi MA, Fallahi F (2021) 'Fiberoptic Bronchoscopy as a Diagnostic Tool in Neonatal Intensive Care Unit: A Single Center Experience'. Iranian Journal of Neonatology 12(1):70–74. https://doi.org/10.22038/ijn.2020.45914.1768
Erdem E, Gokdemir Y, Unal F, Ersu R, Karadag B, Karakoc F (2013) Flexible bronchoscopy as a valuable tool in the evaluation of infants with stridor. Eur Arch Otorhinolaryngol 270(1):21–25
Elmeazawy R, Fasseeh NA, Mubarak AA, Abdelrazik AM, Elsawy NM (2020) Prevalence of expiratory central airway collapse in children undergoing flexible fiberoptic bronchoscopy. N Y Sci J 13(2):33–37
Lee Y-S, Tsao P-C, Jeng M-J, Soong W-J (2018) The comorbidities and risk factors in children with congenital airway anomalies: a nationwide population-based study in Taiwan. Medicine 97(18):e0561
Midyat L, Çakır E, Kut A (2012) Upper airway abnormalities detected in children using flexible bronchoscopy. Int J Pediatr Otorhinolaryngol 76(4):560–563
Guillemaud JP, El-Hakim H, Richards S, Chauhan N (2007) Airway pathologic abnormalities in symptomatic children with congenital cardiac and vascular disease. Arch Otolaryngol Head Neck Surg 133(7):672–676
Acknowledgements
None.
Funding
The authors declare that this study has received no fnancial support.
Author information
Authors and Affiliations
Contributions
Nader Abdelmoneim Faseeh conception, supervision, literature review, and critical review. Mohamed Saeed Abougabal conception, design, supervision, analysis, literature review, and critical review. Marwa Mohamed Farag conception, writing the protocol of the study. Lina Mortada Abdellah data collection, analysis and interpretation, literature review, and writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Research and Ethics committee of Alexandria Faculty of Medicine and consent was taken from all subjects.
Consent for publication
Not applicaple.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abdellah, L.M., Faseeh, N.A., Abougabal, M.S. et al. Retrospective study of congenital airway malformations detected by flexible fiberoptic bronchoscopy in Alexandria University Children’s Hospital. Egypt J Bronchol 17, 31 (2023). https://doi.org/10.1186/s43168-023-00208-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00208-3